A working model of this patient’s cancer, built before the first dose. GeneSilico turns every available input (molecular, pathological, radiological, and clinical) into one computational picture, then reasons over it to surface therapies matched to their own biology and the evidence.
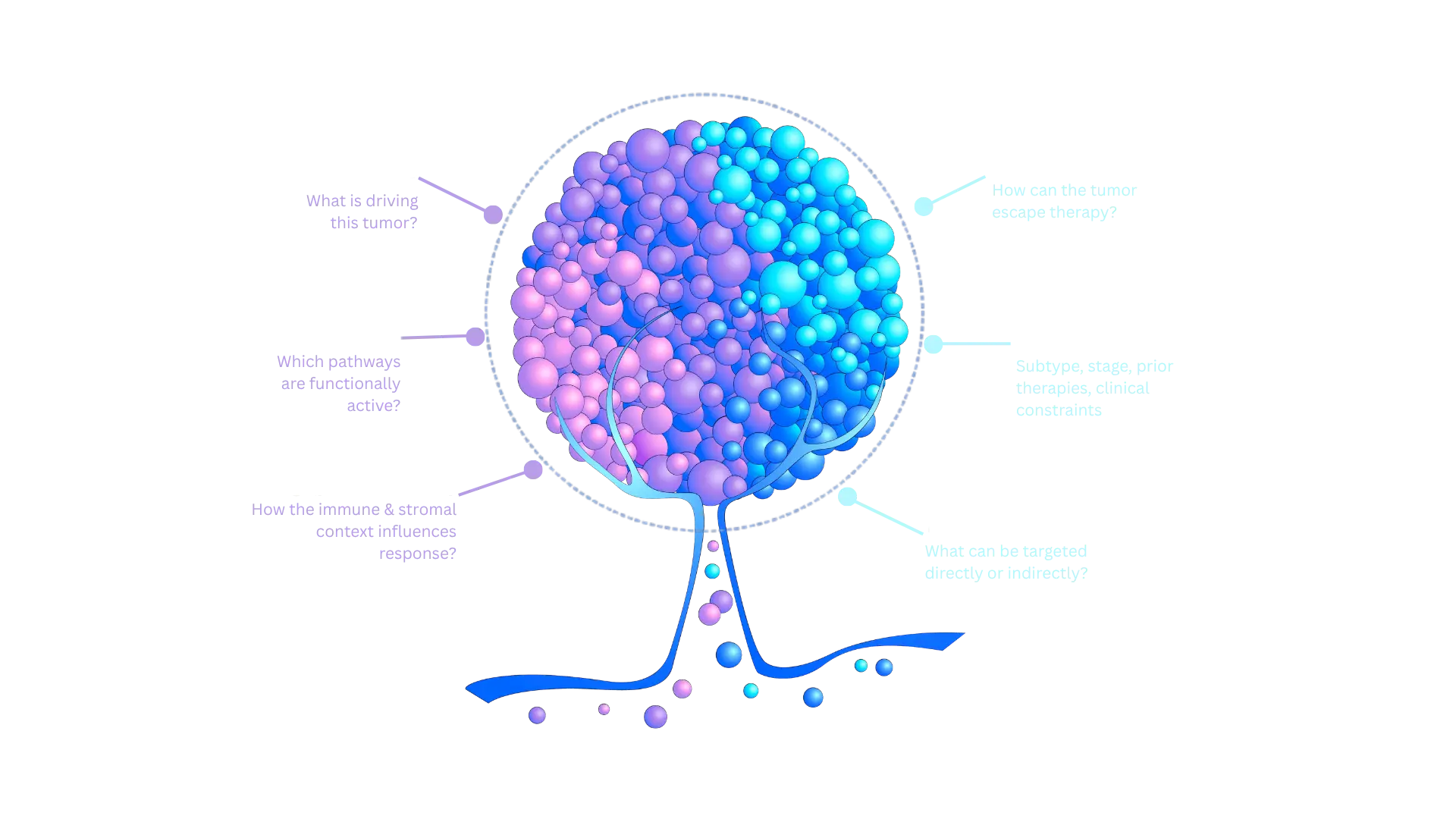
The twin is multi-modal first and multi-omics where present, built from the data a patient actually has. It models not just what the tumor is, but how it responds, resists, and evolves.
Somatic variants, copy number, and structural changes from sequencing or panels.
Pathway activity and tumor micro-environment data from RNA expression.
IHC, histology, and report findings read into structured biomarkers.
Imaging-derived disease extent and metastatic sites.
Diagnosis, staging, prior lines, comorbidities, and performance status.
Every modality a patient has is integrated into a single in-silico model to be read, questioned, and acted on.
Inputs and outputs shown; internal processing is proprietary. Built only on publicly available, openly-licensed knowledge.
Six specialized agents converge on a single patient. Each runs independent analysis and contributes one part of the personalized evidence battery.
Each candidate therapy is scored on a single, consistent scale that blends what the patient's own biology suggests with what published evidence and guidelines support.
The patient's molecular and tumor biology
Strength of published, real-world evidence
Alignment with clinical guidelines
Safety against history and comorbidities
A 54-year-old with HR+/HER2− breast cancer. Before reasoning about what comes next, her twin rebuilds the full disease chronology from every report on file.
Her twin ranks every therapy on the same scale, shows the reasons behind each, and carries the evidence so the rationale can be checked line by line.
Illustrative example. Scores, levels, and rankings shown are for demonstration only and do not represent a clinical recommendation.
For Jane, the report does not stop at “PIK3CA mutated.” It lays out the actionable flow:
gate on the result,
branch, act, and plan the next move.
tumor or ctDNA
biomarker-matched, on-label after progression
next-line option per current guidelines
plan the following line before it is needed
safety tracked as the line proceeds
tumor or ctDNA
biomarker-matched, on-label after progression
next-line option per current guidelines
plan the following line before it is needed
safety tracked as the line proceeds
Conventional reports hand back biomarkers and stop. The Digital Twin Report shows its reasoning, and lets you check it.
An explicit if/then flow: not just what to do, but what next, and when.
The full disease chronology, reconstructed and placed in context.
Every therapy considered is shown, ranked or demoted, each with the reason why.
Where DNA, RNA, pathology and clinical data agree or conflict, surfaced explicitly.
Each recommendation carries its evidence and a confidence level, so the rationale can be checked line by line.
Emerging resistance is surfaced, and what's missing is named as a diagnostic gap with the test that would close it.
All available patient data harmonized and structured for the Digital Twin.
Representing the tumor’s biology and the patient’s constraints.
Plausible therapies proposed, re-searched, and scored.
An evidence-graded list delivered to the oncologist for decision support.
The twin is rebuilt as new evidence and outcomes arrive.
The reasoning approach — a constrained, evidence-first agent — outperformed agents equipped with 200+ tools across five cancer types in a peer-reviewed study.
Decision support for a qualified oncologist, not autonomous decision-making.
Built only on publicly available, openly-licensed knowledge sources.
Coverage depends on the data a patient has; gaps are flagged, never hidden.
Request a demo, or explore how each part of the platform delivers the Digital Twin into your workflow.